Glutathione 1500mg: Dosage, Evidence, and Safe Use Guide
TL;DR:
- Most clinical studies of glutathione use doses between 250mg and 1000mg daily, which reliably increase cellular glutathione levels. The 1500mg dose exceeds current human research evidence and relies mainly on safety data from animal studies. Formulation type, such as liposomal or S-acetyl, significantly enhances absorption, making lower doses more effective than standard forms at higher doses.
A 1500mg daily oral dose of glutathione has become a popular target among wellness enthusiasts and researchers alike, yet clinical trials have largely studied doses in the 250 to 1000mg range. This gap between what most people take and what science has directly examined leaves many users navigating incomplete information. This article translates the available evidence into a practical framework, covering the biological rationale for glutathione supplementation, how the 1500mg dose compares to studied ranges, the critical role of formulation, safety considerations, and actionable decision steps for health-conscious individuals and professional researchers.
Table of Contents
- What is glutathione and why might you consider a high dose?
- How does the 1500mg glutathione dose compare to clinical research?
- Bioavailability breakthroughs: Why formulation determines your real dosage
- Risks, side effects, and expert insights for high-dose glutathione
- Practical guidelines: Is 1500mg glutathione right for you?
- Perspective: What most users get wrong about high-dose glutathione
- Explore quality compounds and research peptide resources
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| High-dose exceeds research | 1500mg is above typical clinical study ranges for oral glutathione supplements. |
| Formulation impacts results | Liposomal and advanced forms dramatically increase absorption and may require lower doses for the same effect. |
| Short-term safety is good | Oral glutathione is generally well tolerated up to 6 months, but long-term, high-dose data is lacking. |
| Personalization is key | Your age, health goals, and genetics determine whether 1500mg is necessary and safe for you. |
| Expert guidance advised | Monitor blood levels if using high doses and seek professional advice for optimal use. |
What is glutathione and why might you consider a high dose?
Glutathione is a tripeptide composed of three amino acids: glutamate, cysteine, and glycine. It is produced endogenously in virtually every cell of the body, with the highest concentrations found in the liver. Its primary roles include neutralizing reactive oxygen species (free radicals), supporting immune function, and facilitating the removal of toxic compounds from the body.
The biological relevance of glutathione extends well beyond simple antioxidant activity. Glutathione enables phase II detoxification in the liver by conjugating with toxins and metabolites, making them water-soluble and easier to excrete. This detoxification pathway is relevant to anyone exposed to environmental toxins, alcohol, medications, or metabolic byproducts of chronic stress.
Key functions that drive supplementation interest include:
- Antioxidant defense: Neutralizes peroxides, heavy metals, and reactive compounds that damage DNA and cell membranes
- Cellular energy support: Protects mitochondria from oxidative damage, which may sustain energy production efficiency
- Immune modulation: Regulates natural killer cell activity and T-lymphocyte proliferation
- Skin health: Inhibits melanin synthesis by suppressing tyrosinase enzyme activity, which explains its growing use in skin brightening protocols
- Detoxification support: Binds and neutralizes heavy metals like mercury and arsenic through conjugation reactions
“Glutathione stores naturally decline with age, chronic illness, and oxidative stress. Supplementation is therefore not purely about adding more of a good thing but about restoring a system under pressure.”
The appeal of higher doses like 1500mg stems from a logical but oversimplified assumption: if some is good, more must be better. Individuals pursuing accelerated recovery from physical training, those undergoing heavy metal detox protocols, or those seeking visible skin brightening outcomes tend to gravitate toward these elevated amounts. Some practitioners also draw parallels to intravenous glutathione use, where higher systemic concentrations are more readily achieved, and assume oral equivalents must match those amounts to produce meaningful effects.
Research on related compounds, such as epitalon research peptide work in anti-aging contexts, reinforces the growing interest in compounds that support cellular resilience, including glutathione as part of an integrated wellness approach.
How does the 1500mg glutathione dose compare to clinical research?
Understanding where 1500mg sits on the evidence spectrum requires looking at what human clinical trials have actually tested. The short answer is that most rigorously conducted human studies have used doses between 250mg and 1000mg per day, and those studies have demonstrated measurable, clinically meaningful outcomes.
A key finding from available clinical trials shows that oral glutathione at doses of 250 to 1000mg daily raised blood and cellular glutathione levels by 30 to 35% after six months of supplementation, without serious adverse events. This is a substantial and biologically significant increase, achieved well below the 1500mg threshold.
| Dose level | Evidence base | Observed effect |
|---|---|---|
| 250mg/day | Multiple human RCTs | Measurable GSH increase in blood and tissue |
| 500mg/day | Human trials, skin studies | Skin brightening, oxidative stress reduction |
| 1000mg/day | Upper range of human clinical data | 30 to 35% rise in GSH stores at 6 months |
| 1500mg/day | Animal safety data only | No direct human efficacy data |
| 10,000mg/day | Theoretical extrapolation | No human data; NOAEL in rats only |
The 1500mg figure does appear in safety literature. Animal studies place the NOAEL (No Observed Adverse Effect Level) for S-Acetyl Glutathione at 1500mg per kilogram of body weight per day in rats. This is a toxicology benchmark, not an efficacy target for humans. Extrapolating from rodent NOAEL data to human dosing recommendations requires significant caution and is not a direct translation.
Statistic callout: Clinical studies confirm oral glutathione at 1000mg/day raises GSH stores by up to 35% in six months. There are currently no published human trials showing superior outcomes at 1500mg compared to 1000mg.
Pro Tip: If you want to work within evidence-based parameters while still using a meaningful dose, 500 to 1000mg per day of a high-quality formulation is better supported than 1500mg. Reserve interest in higher doses for contexts where a qualified researcher or practitioner is actively monitoring outcomes.
Research into other bioactive compounds, including AOD 9604 research and sermorelin for research applications, follows similar principles: the most credible use cases stay within dose ranges that human studies have actually examined.
Bioavailability breakthroughs: Why formulation determines your real dosage
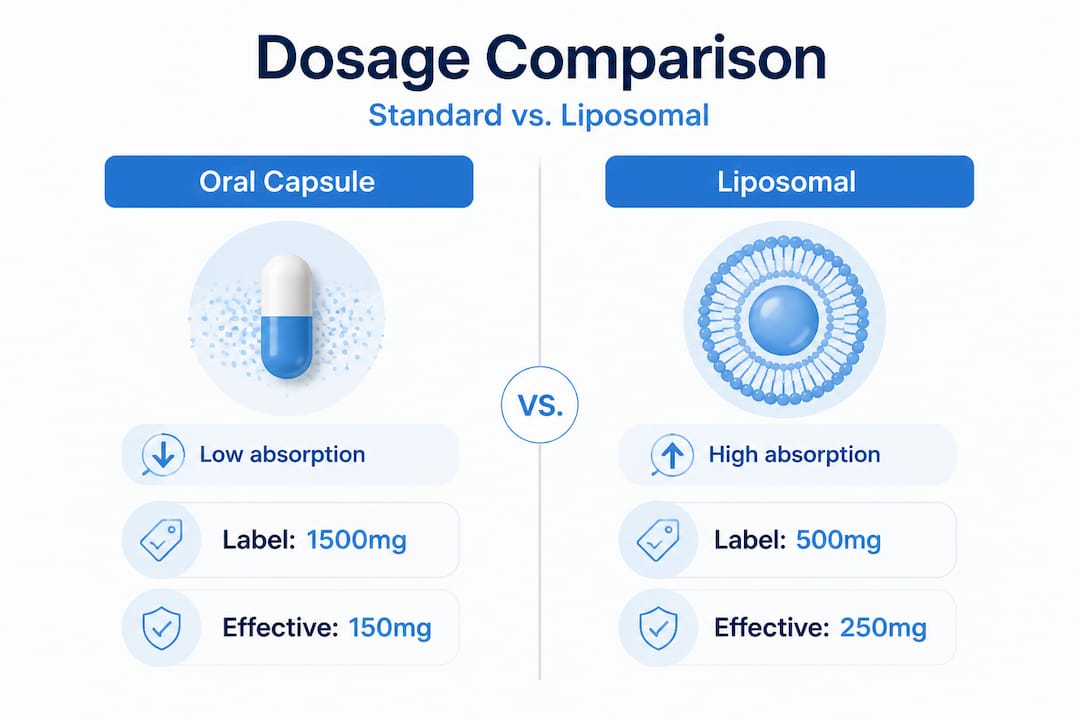
One of the most underappreciated factors in glutathione supplementation is that the dose printed on the label tells only part of the story. What actually reaches your cells depends on the formulation type, and the difference between standard oral glutathione and advanced delivery systems is substantial.

Standard oral glutathione is notoriously difficult to absorb intact. The digestive system breaks the tripeptide down into its constituent amino acids before it can be absorbed into circulation, which limits the amount that ultimately reaches target tissues. Standard oral bioavailability falls below 10 to 30%, depending on the formulation and individual gut physiology.
| Formulation type | Estimated bioavailability | Effective dose equivalent |
|---|---|---|
| Standard oral capsule | 10 to 30% | 1000mg label = 100 to 300mg absorbed |
| S-Acetyl Glutathione | 40 to 60% | Resists GI breakdown; better tissue uptake |
| Liposomal glutathione | 60 to 80% | 250 to 500mg may equal 1000mg standard |
| Intravenous (IV) | ~100% | Bypasses GI entirely |
Liposomal technology encases glutathione molecules within phospholipid bilayers, essentially the same material that makes up human cell membranes. This protects the peptide from enzymatic degradation in the gastrointestinal tract and facilitates direct uptake into cells. The result is that liposomal glutathione at lower doses can match or exceed the cellular effects of much higher doses of standard forms.
Key practical implications of formulation choice:
- A 250 to 500mg liposomal dose may deliver equivalent cellular glutathione levels to 1000mg or more of standard oral glutathione
- S-Acetyl Glutathione resists gastrointestinal breakdown because the acetyl group protects the molecule until it enters the cell, where it is converted to the active form
- Reduced glutathione (the most common standard form) is highly susceptible to oxidation and enzymatic cleavage before absorption
- Sublingual delivery offers an alternative route with moderate bioavailability improvement over standard capsules
Pro Tip: Before concluding that 1500mg is necessary, evaluate whether switching from a standard oral form to a liposomal or S-acetyl formulation would produce equivalent or better results at a fraction of the dose. This approach is more cost-effective, aligns better with available clinical data, and reduces potential risk from high-dose supplementation.
This principle, that delivery mechanism matters at least as much as raw dosage, applies across the broader landscape of research compounds. The quality and form of a compound consistently outweigh the quantity when the underlying biology is properly understood.
Risks, side effects, and expert insights for high-dose glutathione
The safety profile of oral glutathione at studied doses is generally favorable, but the picture becomes less clear above 1000mg per day, and particularly for long-term use. A careful reading of the available safety data reveals both reassuring findings and meaningful caution points.
- Mild gastrointestinal effects are the most commonly reported side effects, including flatulence and loose stools, and these typically resolve with continued use or dose adjustment.
- Hepatic risk with IV administration is documented at high intravenous doses, highlighting that route of administration significantly affects the risk profile.
- Short-term oral safety appears sound for up to six months at studied doses, but long-term data for any dose above 1000mg remains limited.
- Zinc displacement has been observed at very high oral doses in some contexts, suggesting that excessive glutathione supplementation could disrupt trace mineral balance over time.
- Redox imbalance is a theoretical concern: extremely high glutathione levels could disrupt the normal oxidative signaling that cells use for immune defense and stress adaptation.
“Expert guidance notes that dose-response plateaus are likely beyond 1000mg daily for most individuals, and that individual factors including age, genetic variants in glutathione synthesis enzymes, and baseline oxidative stress levels should shape personalized dosing decisions.”
According to expert-reviewed dosing analysis, the assumption that higher doses consistently produce proportionally greater effects is not supported by available data. The relationship between oral dose and cellular glutathione elevation is not linear, particularly beyond 1000mg.
There are specific populations who should avoid high-dose glutathione supplementation or use it only under clinical supervision:
- Individuals with asthma, particularly with inhaled glutathione (bronchoconstriction risk)
- Pregnant or breastfeeding individuals (insufficient safety data)
- Those on chemotherapy, since some protocols depend on controlled oxidative stress to target cancer cells
- People with known genetic polymorphisms affecting glutathione synthesis or recycling
High-dose edge cases are still being mapped in the literature, and the absence of reported overdose toxicity in oral use is reassuring but should not be interpreted as blanket safety for all individuals at all doses.
Pro Tip: If you plan to use glutathione above 1000mg daily for longer than a few weeks, baseline and follow-up blood testing for plasma glutathione, zinc, and liver enzymes provides a safety net and allows evidence-based dose adjustments.
For researchers exploring compounds that interact with metabolic and cellular oxidative pathways, understanding the risk boundary for each compound is critical. Resources on 5-Amino-1MQ metabolic research illustrate how compounds affecting cellular energy metabolism intersect with antioxidant systems in ways that require careful monitoring.
Practical guidelines: Is 1500mg glutathione right for you?
Deciding whether 1500mg glutathione is appropriate for a specific individual or research context requires more than scanning a dosage chart. Several individualization factors should be assessed before committing to an above-evidence dose.
Step-by-step approach for considering 1500mg glutathione:
- Assess your starting point. Measure baseline plasma or whole blood glutathione levels if possible. Individuals with significantly depleted levels due to chronic illness or heavy toxin exposure may have more to gain from aggressive repletion.
- Select the right formulation first. If you are using standard oral glutathione, upgrading to a liposomal or S-acetyl form before increasing dose is the more evidence-aligned strategy.
- Start at 500mg and escalate gradually. Beginning at 500mg per day allows the body to adapt and gives you a clear reference point for evaluating response.
- Monitor subjective and objective markers. Track energy levels, skin appearance, recovery time after exertion, and any digestive symptoms. Objective blood testing at 8 to 12 weeks provides cleaner data.
- Escalate only if needed. If 500 to 1000mg produces no discernible benefit after 8 to 12 weeks and blood levels remain low, an increase toward 1500mg may be considered with clinical oversight.
- Set a review timeline. Reassess at three and six months to determine whether the current dose is producing meaningful changes and whether any safety concerns have emerged.
Individual factors including age, stress levels, and genetic variants in glutathione-related enzymes such as glutathione S-transferase significantly affect both the need for supplementation and the dose required to produce measurable results.
Factors that may increase individual glutathione requirements include:
- Advanced age: Endogenous synthesis declines progressively after age 40
- Chronic oxidative stress: High-intensity training, inflammatory conditions, or significant environmental toxin exposure increases consumption
- Genetic enzyme variants: Polymorphisms in GSTM1 and GSTT1 reduce natural detoxification efficiency
- Nutritional deficiencies: Low selenium, vitamin B2, or cysteine intake limits glutathione recycling and synthesis
- Medication use: Acetaminophen, statins, and some antibiotics deplete glutathione stores
Researchers reviewing compound safety and dosing principles can find additional context in guides covering risks and mechanisms of research compounds and the MOTS-c guide, both of which illustrate how personalized, monitored protocols outperform blanket high-dose approaches across compound classes.
Perspective: What most users get wrong about high-dose glutathione
There is a persistent belief in the wellness community that maximal dosing produces maximal results. With glutathione specifically, this assumption is particularly problematic because it conflates pharmacological logic with a fundamental misreading of how antioxidant systems actually function.
The body does not treat glutathione like a fuel that needs to be continuously topped up beyond its saturation point. Cellular glutathione is tightly regulated through enzymatic synthesis, recycling via glutathione reductase, and export mechanisms. Flooding the system with oral doses far above what can be absorbed and incorporated does not override these controls. It largely results in excretion of unabsorbed material or breakdown into constituent amino acids that the body then redistributes through general metabolic pathways.
The more sophisticated approach, and the one that actually aligns with clinical evidence, focuses on improving the efficiency of delivery before escalating the dose. A researcher who switches from 1000mg of standard glutathione to 500mg of liposomal glutathione is not cutting their dose in half. They may be doubling the amount that actually reaches target tissues. This is the kind of thinking that separates evidence-informed supplementation from dose-escalation guesswork.
Another overlooked variable is timing and cofactor support. Glutathione recycling depends on NADPH (produced via the pentose phosphate pathway), and its synthesis requires adequate cysteine, which is often the rate-limiting precursor. Supplementing with N-acetyl cysteine (NAC) or alpha-lipoic acid alongside glutathione can enhance endogenous production and recycling, potentially producing better results than simply increasing the glutathione dose itself.
The same evidence-critical lens applies when reviewing any research compound. The AOD 9604 dosage analysis illustrates how working within studied parameters, rather than extrapolating to higher doses, consistently produces more reliable and interpretable outcomes. The principle holds for glutathione: more is not a strategy.
For health-conscious individuals and professional researchers, the practical takeaway is clear. Invest in higher-quality formulations, support the body’s own glutathione recycling machinery, and track outcomes with measurable data. That approach will outperform a higher-dose, lower-quality protocol every time.
Explore quality compounds and research peptide resources
For researchers and health-focused individuals who want reliable access to well-characterized compounds, sourcing and quality matter as much as dosing decisions.
Peppy&Me supports both individual researchers and business partners through a transparent, third-party tested research peptides platform with traceable lot and batch numbers from manufacturer to warehouse. Whether you are exploring glutathione-adjacent metabolic compounds, reviewing safety literature, or building a research portfolio, the platform’s resources are structured to support informed decisions. For entrepreneurs and practitioners looking to scale, the private label research peptides partnership program offers backend fulfillment through a trusted quality system. You can also review sourcing standards in detail through guides like safe sourcing for tirzepatide, which applies the same quality criteria relevant to all research-grade compounds.
Frequently asked questions
Is 1500mg of glutathione safe to take daily?
1500mg oral glutathione is above typical human study levels but appears safe short-term for most healthy adults; however, long-term safety at this specific dose is not yet well established in clinical literature.
Does taking 1500mg glutathione help detoxification?
Glutathione supports liver detoxification through phase II conjugation, but no direct research confirms that 1500mg produces greater detox benefits than doses at or below 1000mg per day.
Are there risks of side effects with high-dose glutathione?
The most commonly reported side effects at high oral doses are mild digestive upset; more significant risks have been documented with IV use, and certain populations including those with asthma or who are pregnant should avoid high doses.
Is liposomal glutathione better than regular for absorption?
Yes. Liposomal bioavailability reaches 60 to 80% compared to 10 to 30% for standard oral forms, meaning a lower labeled dose can deliver comparable or superior cellular levels.