Semax Dosage Research: What Researchers Need to Know
TL;DR:
- Semax dosage varies depending on research goals, with nootropic use typically ranging from 200 to 600 mcg per day. Its variants, like N-Acetyl Semax Amidate, are significantly more potent and require lower doses to achieve similar effects, but exceeding 1000 mcg offers no additional benefits and increases side effects. Proper cycling, precise administration, and cautious dosing, along with high-quality storage, are essential for safe and effective research outcomes.
Semax dosage research sits in a frustrating gray zone: dosing figures circulate widely online, yet most lack the clinical grounding that researchers and serious health enthusiasts require. The compound, a synthetic analog of the adrenocorticotropic hormone fragment ACTH(4-10), has a documented clinical history in Russia, but no large-scale Western RCTs exist to confirm what those numbers actually mean for a diverse population. This article cuts through the noise with evidence-based dosage ranges, variant-specific protocols, pharmacokinetic considerations, and a clear-eyed look at safety, so you can approach Semax research with both precision and appropriate caution.
Table of Contents
- Key takeaways
- Semax dosage research: pharmacology and mechanism overview
- Dosage ranges by goal and variant
- Pharmacokinetics and dose-response relationships
- Safety profile and precautions
- Practical dosing strategies for researchers
- My perspective on interpreting Semax dosage research
- Research-grade Semax from a trusted source
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Dosage varies widely by goal | Nootropic use starts at 200–600 mcg/day; neuroprotective protocols can reach 1,000–6,000 mcg/day under clinical conditions. |
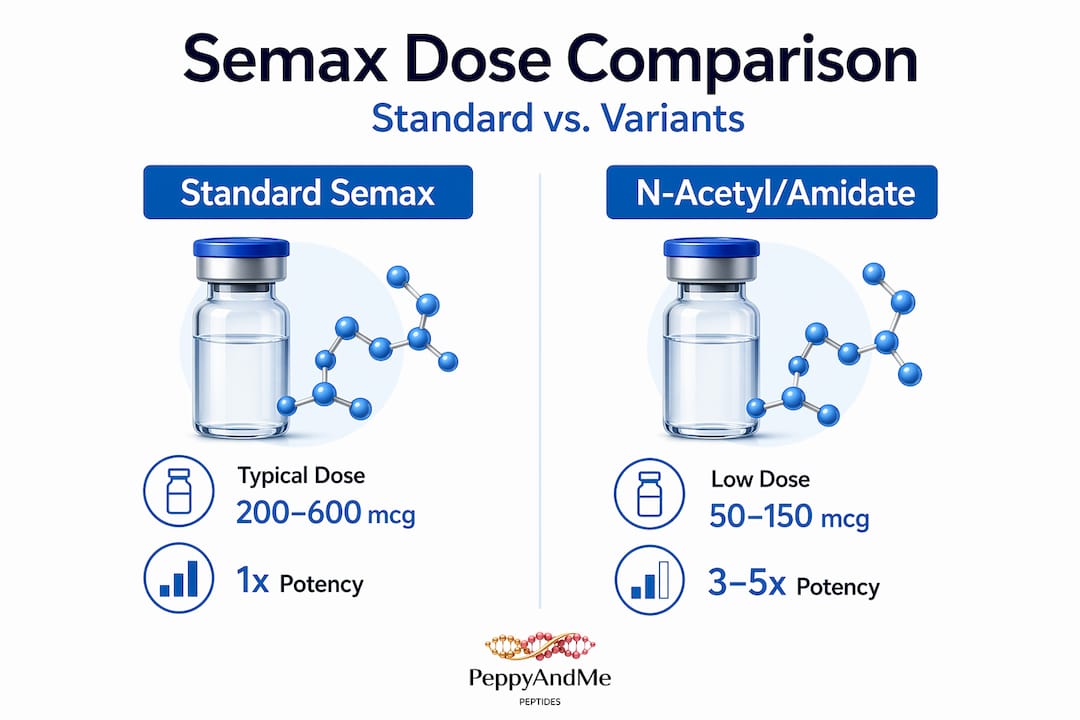
| Variant potency demands dose adjustments | N-Acetyl Semax Amidate is roughly 3–5x more potent than standard Semax, requiring proportionally lower doses. |
| Dose-response plateaus at 1,000 mcg | Exceeding 1,000 mcg per administration does not increase cognitive benefits and raises side effect risk. |
| Cycling protects receptor sensitivity | Structured 10–14 day courses with breaks preserve neurotrophin responsiveness better than continuous use. |
| Storage quality determines potency | Methionine oxidation silently degrades Semax; cold, light-protected storage is non-negotiable for research validity. |
Semax dosage research: pharmacology and mechanism overview
Understanding what Semax actually does at the molecular level is the prerequisite for interpreting any dosage recommendation. Semax is a heptapeptide derived from the ACTH(4-7) sequence with a Pro-Gly-Pro extension added to improve metabolic stability and extend activity. Unlike full-length ACTH, it carries no steroidogenic activity, meaning it does not stimulate cortisol production, which is a distinction that matters considerably when designing research protocols.
Delivery is almost exclusively intranasal. The nasal mucosa provides a direct pathway to the cerebrospinal fluid, effectively bypassing the blood-brain barrier and allowing central nervous system concentrations that oral administration simply cannot match. This route of administration is not incidental. It is the mechanism that makes clinically meaningful dosing at microgram levels physiologically coherent.
At the receptor and cellular level, Semax exerts its primary effects through several converging pathways:
- BDNF upregulation: A single intranasal dose elevates BDNF protein 1.4-fold and BDNF mRNA 3-fold in the rat hippocampus. Brain-derived neurotrophic factor is the key mediator of synaptic plasticity and neuronal survival, which directly underlies the cognitive benefits attributed to Semax.
- Dopaminergic modulation: Semax potentiates dopamine and serotonin turnover in limbic regions, contributing to its observed anxiolytic and mood-stabilizing effects in research subjects.
- Neuroprotective signaling: Semax activates neuroprotective gene expression cascades relevant in models of ischemia and oxidative stress, which is why Russian clinical applications have focused significantly on stroke recovery.
Three Semax variants are currently available for research:
- Standard Semax: The baseline reference compound.
- N-Acetyl Semax: Approximately 2–3 times more potent than the standard form due to enhanced receptor binding affinity.
- N-Acetyl Semax Amidate: The most potent variant, estimated at 3–5 times the activity of standard Semax, with the amide modification providing additional metabolic resistance.
Regulatory context matters here. Semax holds pharmaceutical approval in Russia for cognitive impairment and stroke recovery, but it has no FDA approval or equivalent Western regulatory standing. That status directly shapes what semax dosage research can look like in Western laboratory settings.
Dosage ranges by goal and variant
This is where most online sources either oversimplify or contradict each other. The dosage picture for Semax is actually more nuanced than a single number, because it depends on the research goal, the specific variant in use, and whether the protocol is structured around short cycles or extended courses.
Standard Semax dosing for cognitive research
For nootropic and cognitive enhancement research, standard nootropic dosing sits at 200–600 mcg/day intranasally, administered in one to three divided doses. Beginners and those establishing baseline tolerance typically start at 100–200 mcg once daily and assess response before titrating upward. This conservative entry point matters not because of severe toxicity risk at low doses, but because individual neurochemical sensitivity varies enough that some subjects report meaningful effects well below the midrange.

Russian clinical practice places nootropic use consistently in the 200–600 mcg/day range across 10–14 day courses, with stroke recovery and neuroprotective protocols scaled considerably higher, from 1,000 to 6,000 mcg/day intranasally, and stroke-specific inpatient protocols reaching up to 12,000 mcg/day (12 mg/day) under supervised conditions. Those upper figures are medical-grade clinical doses, not appropriate starting points for independent research.
Variant-specific dose adjustments
The potency differences between Semax variants are not marginal. Treating N-Acetyl Semax Amidate as dose-equivalent to standard Semax is one of the most common and consequential errors in self-directed research.
| Variant | Relative Potency | Typical Research Dose Range | Notes |
|---|---|---|---|
| Standard Semax | 1x (baseline) | 200–600 mcg/day | Most studied; established in Russian literature |
| N-Acetyl Semax | 2–3x | 100–300 mcg/day | Enhanced binding; reduce dose proportionally |
| N-Acetyl Semax Amidate | 3–5x | 50–150 mcg/day | Highest potency; significant overstimulation risk if underdosed carelessly |
The acetyl and amidate modifications extend the half-life and improve receptor binding efficiency. Researchers working with the amidate form should treat it as a different compound for dosing purposes, not simply a stronger version of standard Semax that can be scaled by the same approach.
Cycling protocols and dose frequency
Structured 10–14 day courses with intervening breaks represent the preferred approach in both Russian clinical protocols and among experienced researchers. The rationale goes beyond simple caution. Preclinical models show diminished neurotrophin responsiveness with continuous uninterrupted administration, suggesting that scheduled breaks maintain receptor sensitivity and preserve the magnitude of BDNF-related effects.
Common dosing frequency within a course includes:
- Single daily administration: Used at lower doses (100–300 mcg) for subjects prioritizing cognitive function support.
- Twice-daily dosing: Used mid-range (200–400 mcg per dose) for more intensive protocols; mornings and early afternoons are preferred to avoid sleep disruption.
- Three-times-daily dosing: Reserved for the upper end of nootropic ranges or clinical research protocols; not recommended without prior tolerance data.
Pro Tip: When working with any Semax variant for the first time, establish a dedicated research log before the first administration. Document dose, timing, administration technique, and any observed effects across the full course. This data becomes the basis for rational dose adjustments in subsequent cycles rather than anecdotal guesswork.
Pharmacokinetics and dose-response relationships
Semax pharmacokinetics present a specific challenge for dosing strategy: the plasma half-life is short, measured in minutes to a few hours at most, yet the downstream neurotrophic effects persist substantially longer. This dissociation between plasma presence and biological action is central to understanding why higher doses do not translate linearly into better outcomes.
What the data shows on dose-response
The dose-response relationship flattens above 1,000 mcg per administration. Research subjects administered doses above this threshold do not demonstrate proportionally greater cognitive benefits compared to those receiving doses in the 300–600 mcg range. What does increase above 1,000 mcg is side effect frequency and intensity, including nasal irritation, agitation, and overstimulation. This plateau represents a genuine ceiling effect, not a dosing limitation that can be overcome by switching formulations.
| Dose Range | Expected BDNF Effect | Cognitive Benefit | Side Effect Risk |
|---|---|---|---|
| 100–300 mcg | Moderate neurotrophin elevation | Mild to moderate | Low |
| 300–600 mcg | Substantial BDNF upregulation | Moderate to strong | Low to moderate |
| 600–1,000 mcg | Near-maximal response | Strong | Moderate |
| Above 1,000 mcg | No additional increase | No added benefit | Elevated |
Stability, metabolism, and storage implications
Semax contains a methionine residue that is highly prone to oxidation, which reduces biological activity without any visible change in the solution. A peptide solution that looks identical to freshly prepared Semax may have meaningfully degraded potency if storage conditions were compromised. Cold storage, minimal oxygen exposure, and protection from light are the three variables that matter most for maintaining research-grade Semax between administrations.
Pro Tip: Reconstituted Semax should be stored in a refrigerator and used within the timeframe specified by the manufacturer. If there is any uncertainty about storage continuity, treat the sample as potentially compromised and consider the implications for data interpretation before proceeding.
Timing implications follow from the half-life and mechanism. Because neurotrophic effects outlast plasma presence, twice-daily dosing does not need to be separated by equal intervals the way pharmacokinetically active drugs do. Morning and midday administrations serve the goal of maximizing daytime neurotrophin availability while minimizing late-evening CNS stimulation that could impair sleep quality and confound cognitive endpoints.
Safety profile and precautions
Semax has a favorable safety record based on its Russian clinical history, but that record must be interpreted within the limits of the evidence base. Researchers working with this peptide need to account for both the documented risks and the gaps in the current literature.
The most commonly documented adverse effects include:
- Nasal irritation: Reported in approximately 10% of users, typically mild and transient. Rotating between nostrils and ensuring proper dilution of the reconstituted solution reduces frequency significantly.
- Blood glucose elevation: Diabetic subjects and those with impaired glucose regulation face a documented risk of elevated blood glucose following Semax administration. Monitoring glucose levels before and after initial administrations is a basic precaution for any subject with a relevant metabolic history.
- Paradoxical agitation and anxiety: Observed rarely but documented, typically at higher doses or in individuals with elevated baseline dopaminergic tone. The mechanism likely relates to Semax’s potentiation of dopamine release in limbic pathways.
- Dopaminergic stimulant interactions: Semax potentiates dopamine release; combining it with amphetamines, methylphenidate, or other dopaminergic stimulants carries real risk of synergistic cardiovascular stimulation and neuropsychiatric adverse effects. This combination should be avoided in research protocols.
- Peptide degradation risk: As discussed, methionine oxidation silently reduces potency, but improperly handled peptides may also introduce sterility concerns. Aseptic reconstitution technique is not optional in research use.
The broader safety context is important to state clearly: no large-scale Western placebo-controlled RCTs exist for Semax. The Russian literature predominates, and it carries inherent limitations including publication bias, combination therapy confounding (Semax is often studied alongside other agents), and clinical populations that may not reflect research subjects in other contexts. Caution is warranted not because of documented severe harm, but because the evidence base does not yet provide the certainty that well-powered randomized trials would.
Reviewing safe peptide research practices before initiating any Semax protocol is a reasonable baseline step that experienced researchers treat as routine.
Practical dosing strategies for researchers
Translating the pharmacology and dosage data into a functional research protocol requires several decisions that go beyond selecting a number from a table. The following recommendations reflect both the research literature and the practical considerations that arise when working with research-grade peptides.
Start at conservative doses. Begin any new research subject on standard Semax at 100–200 mcg once daily for the first three to five days. This serves as a tolerance assessment phase that identifies paradoxical responders, unusual sensitivity, or logistical issues with administration before committing to a full dosing cycle.
Use structured cycles, not continuous administration. Schedule 10–14 day active periods followed by breaks of equal or greater length. This approach preserves receptor sensitivity and reflects the cycling protocol used in Russian clinical practice that produced the outcomes described in the literature.
Adjust doses downward for potent variants. If transitioning from standard Semax to N-Acetyl Semax or N-Acetyl Semax Amidate, reduce the dose proportionally from the outset. The 3–5x potency of the amidate form means a 200 mcg dose of standard Semax translates to roughly 40–67 mcg of the amidate variant.
Standardize intranasal administration technique. Hold the head slightly forward, administer into one nostril while occluding the other, and breathe gently through the nose after administration. Consistency in technique reduces variability in absorption and improves the reliability of dose-response observations.
Verify peptide quality and storage history. Source Semax only from suppliers who provide third-party certificates of analysis confirming purity, mass accuracy, and sterility. Review peptide handling guidance to establish proper storage and reconstitution protocols before the first use.
Avoid known interaction risks. Remove stimulant compounds with dopaminergic activity from concurrent use during Semax research cycles. Document all concurrent substances in research logs for accurate interpretation of outcomes.
Pro Tip: Keep a research log that tracks dose, time of administration, concurrent compounds, and qualitative observations for every session. After a full cycle, review the log before adjusting the protocol. This documentation practice transforms anecdotal experience into usable data and supports rational decisions for subsequent cycles.
My perspective on interpreting Semax dosage research
The challenge I see most often in this field is researchers lifting dose numbers from Russian clinical trials and applying them directly to independent research contexts, without accounting for the methodological gap between that literature and the standards Western researchers are trained to require.
In my experience, the single most underappreciated variable in Semax research is the absence of standardized Western-context evidence. Russian approval is real, and the mechanistic case for Semax’s effects is compelling. But clinical use in Russia often involves supervised settings, combination protocols, and patient populations that differ from the independent researcher or health enthusiast working with a reconstituted solution in a laboratory or home environment.
What I’ve found is that patience with conservative dosing and respect for cycling protocols produces more meaningful research outcomes than chasing higher doses. The dose-response plateau above 1,000 mcg is one of the most reliable findings in the literature, and I’ve seen researchers repeatedly ignore it in the belief that more is more. It isn’t. With Semax, consistency within the evidence-supported range produces better data than intensity at doses that exceed what the neurotrophin response can actually translate into observable benefit.
The variant potency issue also deserves more attention than it typically receives. Treating N-Acetyl Semax Amidate as interchangeable with standard Semax because they share a name is an error with real consequences for both data quality and subject safety.
My recommendation is to treat Semax dosage research as a long-term project rather than a single experiment. Document carefully, cycle responsibly, and resist the pull toward protocols that sound compelling on forums but have no grounding in the clinical or preclinical record.
— ELAIZA
Research-grade Semax from a trusted source
For researchers who take dosing precision seriously, the quality of the source material is as consequential as the protocol itself. Peppyandme provides research-grade peptides with third-party verification covering purity, mass accuracy, endotoxins, sterility, and heavy metals. Every product carries traceable lot and batch numbers from manufacturer to warehouse, so sourcing decisions are grounded in documented evidence rather than vendor claims.
Peppyandme’s platform also includes built-in research support tools, including a dose calculator for precise measurement guidance and an extensive peptide glossary covering protocols and handling practices. Researchers can explore the full research peptide catalog to review available Semax variants and confirm product specifications before ordering. For those new to peptide research or looking to formalize their protocols, the platform’s peptide handling resources and lab practices guide provide a structured foundation. Same-day shipping on orders placed before 2 PM and real-time customer support make the logistics of research supply management straightforward, so focus stays on the research itself.
FAQ
What is the standard Semax dose for cognitive research?
Standard nootropic dosing is 200–600 mcg/day intranasally, with beginners starting at 100–200 mcg once daily to establish tolerance before titrating upward within the evidence-supported range.
How does N-Acetyl Semax Amidate dosing differ from standard Semax?
N-Acetyl Semax Amidate is approximately 3–5 times more potent than standard Semax, requiring proportionally lower doses, typically 50–150 mcg/day, to avoid overstimulation while achieving comparable neurotrophin effects.
Why does Semax dosage above 1,000 mcg not improve cognitive outcomes?
The dose-response relationship plateaus above 1,000 mcg per administration; beyond this threshold, cognitive benefits do not increase while side effect risk does, making consistency and cycling within the effective range more productive than dose escalation.
What are the main side effects researchers should monitor?
The most commonly documented effects include nasal irritation in approximately 10% of users, potential blood glucose elevation in diabetic subjects, and rare paradoxical agitation, particularly when Semax is combined with dopaminergic stimulants.
How should Semax be stored to maintain research validity?
Semax should be stored in cold, light-protected conditions immediately after reconstitution, because methionine oxidation reduces biological activity without visible changes to the solution, making compromised storage a silent source of unreliable research data.